Social Determinants Digest: Institutions and racial disparities over time
Sociologist Alford A. Young, Jr., Ph.D., wrote a seminal article titled “The Character Assassination of Black Males: Some Consequences for Research in Public Health. Here, Young finds that the cornerstone of social inequity is the conglomeration of beliefs and attitudes of worthiness, desirability, and character. He argues that the social consequences of racism amount to an “extreme form of character assassination,” and that any new public health agenda to achieve equity must mitigate character assassination and shift the public imagination.
But if racism is merely the sum of encounters between individuals, their beliefs and actions towards another, then how do we explain racial disparities that persist over time? How do we explain a systematic, institutionalized practice of weathering worthiness, disclaiming desirability and maligning character not only of Black men but Black people at large in the U.S.?

Sociologist Loic Wacquant, Ph.D., and public health expert Gregorio A. Millet, MPH, can help answer this question. In an article, “From Slavery to Mass Incarceration,” Wacquant offers a structural analysis of four peculiar institutions that have “operated to define, confine, and control African Americans in the history of the U.S:”
1) Slavery (246 years)
Established the provision and control of labor, created a racial caste system, informed the ideology of race with biological dimension (see One-Drop Rule and hypodescent) and reduced the slave to 3/5ths of a man within the U.S. Constitution.
2) Jim Crow (100 years)
Emancipation presents the dilemma of how to maintain both a proximity to labor and a symbolic distance to prevent caste erosion by amalgamation. Jim Crow circumscribed the lives of formerly enslaved people while binding them to former enslavers in a dynamic of perpetual submission.
3) Ghetto (53 years)
Emerges while a mass migration to flee Jim Crow in the South ensues, and it is no less totalizing and restricting: Social equality is firmly denied and economic marginality persists. Securing voting and civil rights forces integration into the law but does not prevent the development of yet another peculiar institution that edifies eroding caste cleavages.
4) Hyperghetto and Prison (53 years and counting)
Prison emerges as a solution to social problems such as poverty and addiction. The ghetto and prison form a “parallel institutional nexus” which locks a racial caste into subordination and dependency. Wacquant describes the U.S. as “the first genuine prison society in history,” and explains that prisons preserve a racial caste system that began with racial slavery.
Wacquant’s work helps us understand why disparities in health along racial lines persist despite our best efforts, and why they would persist even if we were to recuperate public images or change the public’s outlook on the character of Black people. It’s because of the systemic and institutional factors that circumscribe their lives that the realities of health inequity and social determinants of health remain unchanged.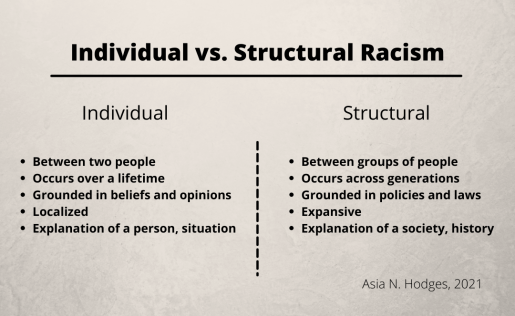
Indeed, many assume that Black communities are no longer suffering from racial oppression as they did during time periods such as slavery and Jim Crow. While there have been structural changes through law, we have ultimately been unsuccessful in eliminating structural racism or its impacts on long-term health equity.
For example, Millet and his team show that there are significantly higher rates of COVID-19 cases and deaths in disproportionately Black counties. Most of these counties are in the southern U.S, a region which also suffers from the highest rates of unemployment and uninsured individuals, while also having limited access to healthcare (for example, failure to adopt Medicaid expansion).
We see the effects of structural racism when we acknowledge that in 1850, most African Americans were enslaved in the southern U.S. This pattern is the result of structural racism, which enables these health disparities to persist.
Here are some ways to begin understanding and combating structural racism:
- Read as a community. Form a reading group with members from clinical care, academic research, and the larger community to engage in conversation related to texts that provide the history and prolonging effects of oppressive systems. This is something we’ve done at Baylor College of Medicine.
- Challenge your workplace to take “diversity, inclusion, and equity” initiatives to the next level. While it is important to have diverse representation, changing the orientation and structure of our institutions from non-racist to anti-racist involves active mentorship and sponsorship, advancement and promotion, and an anti-racist work environment for people of color.
- Be engaged in policy. Know your local and state elected officials. When racist policies and laws (those which create or sustain inequity among racial groups) are being considered, contact those officials to advocate for equity.
- Find a local organization (or create your own) that is involved in addressing health and social disparities (e.g., food pantries, housing services). Commit to serving with an organization regularly.
If you are interested in learning about more opportunities related to these four areas, including Houston-based organizations or recommendations for reading groups, please contact us. We realize that this work requires time and energy, but we all must make a commitment to combating racism. Together we can make a difference.
–By Asia Hodges, student in the post-baccalaureate program at Baylor College of Medicine who is also obtaining a Master’s degree in Microbiology from the University of Florida, and Bailey Martin-Giacalone, third-year graduate student at Baylor College of Medicine