Molecular profiling of meningioma hints at tumor behavior
Meningiomas, the most common primary brain tumors, are typically benign. One-fifth of them, however, recur despite complete surgical removal. Reliably predicting whether a patient’s tumor will recur has not been easy. The current meningioma classification, the only means available to predict tumor recurrence, does not consistently foresee whether a tumor will return.
Dr. Akash J. Patel, a neurosurgeon specialized in treating meningioma at Baylor St. Luke’s Medical Center, knows firsthand of the need to provide patients with an improved prognosis. He and Dr. Tiemo Klisch, in collaboration with Dr. Huda Y. Zoghbi and other colleagues, took on the project of finding a more reliable tool to predict tumor recurrence.
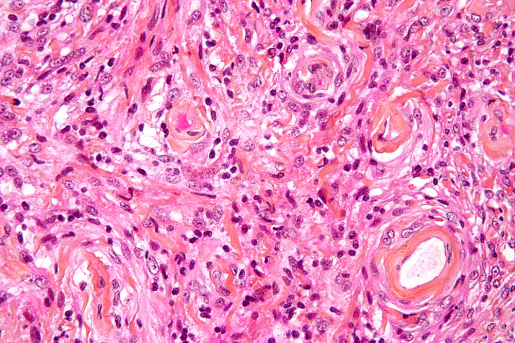
“The current classification is the World Health Organization system. It divides meningiomas into three categories: WHO grade I (benign), grade II (atypical) and grade III (malignant). The WHO system is based on tumor histopathology; that is, the appearance of tumor cells under the microscope,” said Patel, who also is an assistant professor of neurosurgery at Baylor College of Medicine and an investigator at the Jan and Dan Duncan Neurological Research Institute at Texas Children’s Hospital.

Although the histopathology system has some success predicting tumor recurrence, there seems to be room for improvement.
“For instance, WHO grade II and III tumors tend to recur, but we also have seen patients with grade II meningioma whose tumors have a more benign course,” Patel said. “On the other hand, a portion of grade I tumors, which are generally cured with surgery, recur despite complete resection and benign microscopic features. It seemed that the way we were looking at meningioma could benefit from reevaluation, and this inspired us to conduct this research.”
Other brain tumors, such as medulloblastoma and glioma, have been redefined based on molecular and genetic features, allowing for improved prognostication and potential therapeutic targets.
“We believed that meningioma might also be amenable to this sort of molecular profiling,” said Patel, who also is a member of the Dan L Duncan Comprehensive Cancer Center.
Digging into meningioma molecular signatures
In the first part of this study, the researchers explored the possibility of identifying meningioma molecular signatures that would enable them to reliably predict the most likely tumor behavior after surgical removal. They looked into the sequences of all protein-producing genes (whole exome sequencing), gene expression and clinical data of 160 meningioma samples WHO grades I, II and III, from 140 patients.

“The molecular data suggested three meningioma types: A, B and C. Type C tumors had a remarkably worse clinical course than types A or B tumors,” said Klisch, assistant professor of molecular and human genetics at Baylor and the Jan and Dan Duncan Neurological Research Institute. “These groups, however, did not directly correlate with the WHO grading system. For instance, the WHO system would classify more than half of the tumors in our C (aggressive) molecular type as type I (benign). We think that using gene expression data might allow for better prediction of tumor behavior.”
Predicting the worst cases
In the second part of this study, Patel, Klisch and their colleagues gained a better understanding of how the worst cases happen. They discovered a unique characteristic of type C (aggressive) meningioma; their DREAM complex is dysfunctional.
“The DREAM complex is like a ‘brake’ for cell division. In type C meningiomas, the DREAM complex is inactive – the brake is not functional. Consequently, cells are not able to regulate cell division properly, which contributes to their malignant transformation,” Klisch said. “We think that dysregulation of the DREAM complex is a key step that in the end leads to the most aggressive behavior in these tumors.”
“This study has two major findings,” Patel concluded. “One is that our results suggest that molecular profiling for meningioma reliably predicts tumor recurrence. The second finding is that we have identified DREAM complex dysfunction as a leading factor in aggressive meningioma.”
“This work shows that combining clinical, pathological and molecular data not only helps reveal whether a tumor is likely to recur, but also provides insight into genes that drive malignant behavior,” said Zoghbi, professor of molecular and human genetics at Baylor, director of the Jan and Dan Duncan Neurological Research Institute and investigator with the Howard Hughes Medical Institute. “More work is needed to refine the molecular signatures of various meningiomas and to gain better understanding of their pathogenesis.”
Interested in all the details of this study? Find them in the Proceedings of the National Academy of Sciences.
Other authors who contributed to this work are Ying-Wooi Wan, Rami Al-Ouran, Jean-Pierre Revelli, Maria F. Cardenas, Mazen Oneissi, Liu Xi, Ali Jalali, John F. Magnotti, Donna M. Muzny, Harsha Vardhan Doddapaneni, Sherly Sebastian, Kent A. Heck, J. Clay Goodman, Shankar P. Gopinath, Zhandong Liu, Ganesh Rao, Sharon E. Plon, Daniel Yoshor and David A. Wheeler.
This study was funded by the Roderick D. MacDonald Fund, the Jan and Dan Duncan Neurologic Research Institute at Texas Children’s Hospital and the Hamill Foundation. Further support was provided by a K08 award from the NINDS (K08NS102474), the Howard Hughes Medical Institute and a P30 Cancer Center Support Grant (NCI-CA125123).