Understanding granulomatous mastitis, a rare breast condition

Granulomatous mastitis (GM) is an episodic breast disease mostly affecting premenopausal women. Patients can have severe symptoms for a while, but then symptoms clear up with or without treatment and the breasts almost return to normal.
What is this mysterious disease that stays around for weeks, months or even years?
Common GM symptoms
The condition ebbs and flows and there’s no way of predicting when symptoms might become more severe. It’s unknown what causes this chronic, episodic inflammation of the breast. In this way, it’s somewhat similar to diseases like rheumatoid arthritis, lupus, and inflammatory thyroid disease (e.g., Grave’s or Hashimoto’s thyroiditis) where the body’s inflammatory cells react to and attack its own tissue, rather than bacteria or fungus.
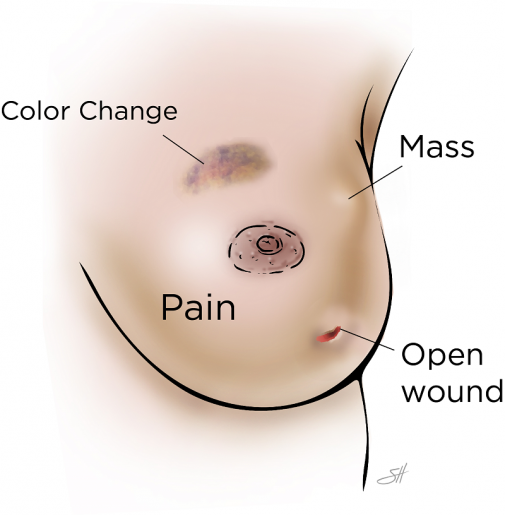
- Mass: Inflammatory tissue (phlegmon) that can grow quite large and feels, sometimes ominously, like a tumor.
- Skin color changes: Patches of darker red, even violet or brownish red skin.
- Open wounds: One or more wounds that can drain thin, watery, mucoid or bloody fluid
- Pain
Mimics other breast diseases
Patients with GM often go to several providers seeking help for these symptoms. It’s common for patients and providers to confuse GM symptoms with symptoms of other conditions. Some clues from the patient’s history and physical exam can help distinguish GM from other breast diseases.
- Inflammatory breast cancer (IBD): This aggressive disease affects the skin as well but is often accompanied by enlargement of the affected breast and can make the breast skin appear like an orange peel (thickened by lymph fluid). IBD skin is often brighter red and less patchy than GM skin, though not always. IBD can be associated with swollen lymph glands in the armpit on the same side as the affected breast. This cancer is best treated with a combination of chemotherapy, surgical removal of the breast and lymph nodes (modified radical mastectomy) and radiation.
- Breast cellulitis: This infection of the breast skin is caused by bacteria that occur naturally on human skin like staph aureus. The skin is often bright red and more painful with less open wounds than GM. This condition is best treated with antibiotics.
- Breast abscess: A more serious, intense infection of the breast. A pus-filled cavity within the breast causes swelling, pain, fever and general malaise (patients usually feel and look sicker than with GM). This discharge is usually thicker and more intensely yellow than GM discharge. This condition is best treated by image-guided aspiration with drain placement.
Diagnosing GM
The best way to diagnose GM is with imaging, usually a breast ultrasound, and an image-guided biopsy. The radiologist can often tell the subtle differences on ultrasound between the inflammatory phlegmon, a cancerous tumor, or a pocket of pus in the breast. The diagnosis is finalized by taking a sample of the tissue using a core needle biopsy gun. Pathologists then analyze this tissue in the lab with a microscope. GM is diagnosed when they see inflammatory cells associated with “granulomas.” Occasionally, other conditions — tuberculosis or sarcoidosis, for example — can cause tissue to look like this under the microscope, so tests are done on patients to rule these out.
Long-term treatment
All GM treatment is symptomatic, like it is for the common cold. There is no cure, and surgery is almost never indicated. Avoiding tobacco, losing weight and controlling diabetes can help. Treatments calm down the body’s overactive inflammation, starting with two to three over-the-counter ibuprofen tablets every six hours. If this proves insufficient, stronger anti-inflammatory medicine like steroids (usually a 30-day course, one tablet a day) or a steroid injection into the phlegmon is used.
It can be difficult to deal with the reality that these cyclical symptoms often stick around for a while. The good news is the disease typically goes away as mysteriously as it came.
-By Brian Lassinger, instructor of surgery and physician assistant in the Michael E. DeBakey Department of Surgery at Baylor College of Medicine