A new mechanism to explain benign prostatic hyperplasia
Benign prostatic hyperplasia (BPH), a non-cancerous enlargement of the prostate, affects about half the men between 51 and 60 years of age, and nine out of 10 men older than 80. How BPH happens, however, is still open for debate.
“Scientists have considered that inflammation can cause BPH. But how inflammation initiates in human prostate tissues and promotes BPH remains unclear,” said senior author Dr. Li Xin, associate professor of molecular and cellular biology at Baylor College of Medicine. “Our study provides molecular insights to answer these questions.”
The researchers who are at Baylor, the University of Texas Southwestern Medical Center at Dallas, UT MD Anderson Cancer Center and the Michael E. DeBakey Department of Veterans Affairs Medical Center, report their findings in Molecular Cell.
In the beginning, “we were investigating the role of the androgen receptor in prostate epithelial cell homeostasis, or how these cells balance their functions to work properly,” said first author Dr. Boyu Zhang, postdoctoral associate in Xin’s lab.
In particular, the scientists were studying the role the androgen receptor plays in prostate homeostasis by deleting the androgen receptor in luminal epithelial cells. The androgen receptor allows cells to respond to androgens, hormones that affect how the male reproductive system develops. Most prostate luminal epithelial cells need androgen to survive. Dihydrotestosterone is the most active androgen.
Although other research groups had already studied the role of androgen receptor in the prostate by deleting the receptor in prostate epithelial cells, Xin and colleagues were not satisfied with the results.
“There are two limitations to those previous studies,” said Xin. “First, their approach was to delete the androgen receptor in the prostate at very early stages of the animal’s development, before puberty. Therefore, it is uncertain whether the outcomes of the experiment reflect the role of androgen receptor in development or the role in homeostasis. The second limitation is that the androgen receptor was deleted in almost all of the epithelial cells, including luminal cells and basal cells. This makes it difficult to determine whether the results are a direct consequence of the cells’ losing their androgen receptor or an indirect outcome of the loss of the receptor.”
Xin and colleagues decided to use a genetically engineered mouse model developed in Xin’s laboratory, which would allow them to delete the androgen receptor in a fraction, as opposed to all, of the prostate epithelial cells. They carried out their experiments in adult mice, not in mice that had not reached puberty.
The results of their experiments serendipitously illuminated a chain of events that can help clarify how inflammation and cell proliferation interact with each other in the prostate and result in BPH.
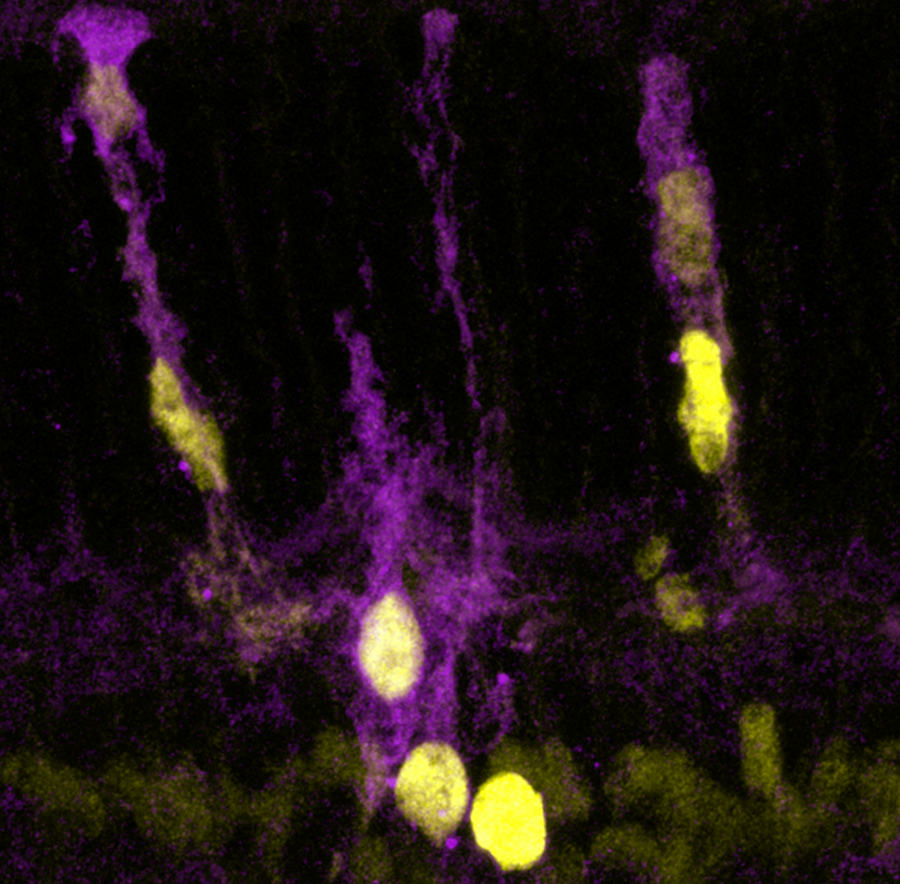
“When we deleted the androgen receptor in a fraction of prostate epithelial cells called luminal cells, the cells produced mediators of inflammation called cytokines, which the luminal cells normally don’t do. Deletion of the androgen receptor also resulted in defects in tight junctions – connections between two adjacent cells that close the space between them,” said Xin. “In normal cells, tight junctions are intact and molecules, such as mediators of inflammation, cannot leak into surrounding areas. But in the luminal cells in which the androgen receptor was deleted, tight junctions were not intact and cytokines produced by the luminal cells could leak into surrounding areas.”
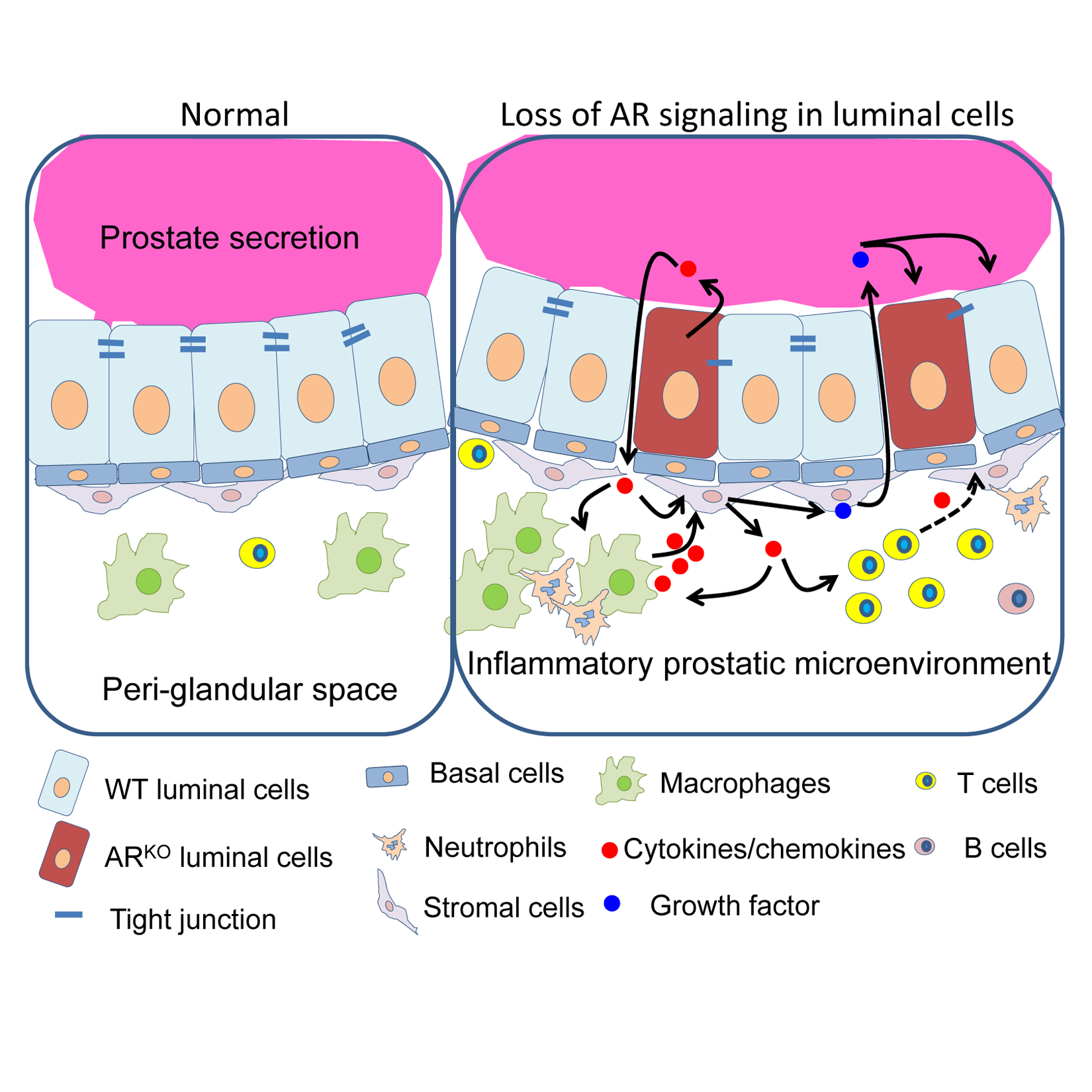
The scientists observed that the ‘leaked cytokines’ promoted the recruitment of immune cells, especially macrophages and T cells, into the prostatic microenvironment. These immune cells then secreted additional cytokines, such as IL-1, that subsequently attracted more immune cells. In addition, IL-1 induced stromal cells to secrete growth factors that stimulated the proliferation of cells in the prostate, including luminal cells and basal epithelial cells.
“In summary, deleting the androgen receptor triggers an inflammatory response that promotes cell proliferation,” said Xin. “In the process, some luminal cells that rely on androgen signaling for their survival will die, but, at the same time, the chain of events creates a signal that promotes luminal cell proliferation. Our result that disruption of androgen receptor signaling in luminal cells can drive inflammation is consistent with the observation that luminal cells of inflamed human prostate glands have fewer androgen receptors than luminal cells from non-inflamed prostates. Our results, however, do not rule out that inflammation can affect androgen receptor expression. It is possible that this is a vicious cycle.”
This research has clinical implications related to the treatment of BPH with androgen-targeting therapy, the goal of which is to deplete androgen to starve proliferating cells that require androgen to survive.
“We unexpectedly identified a mechanism that may explain resistance to androgen-targeting therapy,” said Zhang.
“Our results may explain why some BPH patients respond to androgen-targeting therapies, such as finasteride, while in other patients the disease continues to progress,” said Xin. “We suggest that treatment for BPH might be more effective if patients received androgen-targeting therapy together with drugs that target inflammation.”
###
Other contributors to this work include Oh-Joon Kwon, Xing Wei, Li Zhang, William Brinkley, Yiqun Zhang, Patricia D. Castro, Mark Titus, Rui Chen, Mohammad Sayeeduddin, Chad J. Creighton, and Michael M. Ittmann. These researchers are affiliated with one or several of the following institutions: Baylor, the Dan L Duncan Comprehensive Cancer Center, the University of Texas MD Anderson Cancer Center and the Michael E. DeBakey Veterans Affairs Medical Center. This study was performed in collaboration with researchers at UT Southwestern Medical Center, Dallas, including Gervaise Henry, Alicia Malewska, Ganesh Raj, Ryan Mauck, Claus Roehrborn and Douglas Strand.
Support for this work was provided by the Cytometry and Cell Sorting Core at Baylor College of Medicine (NIH grants AI036211, CA125123, and RR024574), and by grants R01DK092202 and R01DK107436, K01DK098277, P20DK097775, and NIH P30 CA125123 (the Cancer Center Shared Resources Grant).